Umbilical hernia
Umbilical hernia i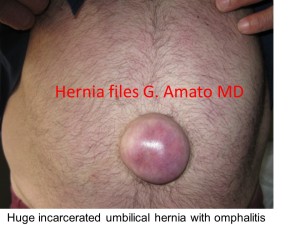 s a bulging of the navel which occurs at all ages and in both sexes. Due to pregnancy, is prevalent in women. It can become very large. Is frequently complicated by inflammation of the skin (Omphalitis) that can cause ulcerations. If ulcer involves the hernia content, infection and/or peritonitis are the consequence. Chronic inflammation of the skin causes hard adhesion brides between the hernia sack and its content, making the surgical procedure more difficult. If the umbilical hernia becomes irreducible a strangulation of the content is the consequence. In this case an emergency intervention is mandatory.
s a bulging of the navel which occurs at all ages and in both sexes. Due to pregnancy, is prevalent in women. It can become very large. Is frequently complicated by inflammation of the skin (Omphalitis) that can cause ulcerations. If ulcer involves the hernia content, infection and/or peritonitis are the consequence. Chronic inflammation of the skin causes hard adhesion brides between the hernia sack and its content, making the surgical procedure more difficult. If the umbilical hernia becomes irreducible a strangulation of the content is the consequence. In this case an emergency intervention is mandatory.
therapy
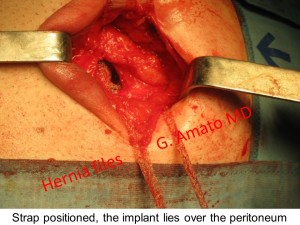
The treatment is surgical. In the case of small hernias primary suture closure is the most practiced. Nevertheless, in case of large umbilical hernia, the suture repair shows a recurrence rate up to 54%. (1) This reason is preferable a prosthetic repair, placing the implant between the peritoneum and the posterior abdominal wall. In order to respect the kinetics of the abdominal wall, a fixation free mesh pla
The Octomesh implant XS, developed by Prof. Amato and a team of physiologists and engineers, eliminates the need for fixation (with sutures or similar). It ensures a very broad coverage of the defect, requires smaller incisions, diminishes the surgical trauma. All in all, it results in a faster and easier procedure. The complication rate is very low and no recurrences are reported in a follow up of 3 years.
the octomesh technique for umbilical hernia repair
The “tentacles” of the Octomesh implant are the key element that allows a huge step forward in terms of safety in  urgical operations and clinical results.
urgical operations and clinical results.
Once positioned the mesh, the “tentacles” are tunneled with a special instrument through the fat tissue under the skin, thus ensuring the mesh an adequate holding force (friction) to keep the implant in place without sutures. In this way, the mesh is perfectly anchored by 8 “tentacles”. While at same day of the procedure it takes 280 gram pull out force to dislodge one strap, 15 days later a traction force greater than 40 kg is needed to remove all the straps.
This type of fixation by friction, without sutures, (“Freexation”) is successfully used since nearly 10 years in procedures for urinary stress incontinence in women, with millions of operations performed today. (1, 2, 3, 4, 5)

benefits for the patient
The advantages for the patient are:
- Small incision, less surgical trauma and better cosmetic results
- Broad coverage of the defect with consequent reduction of the possibility of recurrence
- Shorter operative procedure
- Low complications rate
- No recurrence, in a follow-up of 3 years
benefits for the surgeon
The advantages for the surgeon are:
- Fixation free procedure
- Easier procedure
- Faster procedure
- Broader coverage of the defect
- Standardized procedure, easy reproducibility (learning curve ca. 5 interventions)
- Reduction of complications compared to conventional implants and no recurrences in a follow-up of 3 years

references
- Amato G. et al. Prosthetic stap system for simplified ventral hernia repair: results of a porcine experimental model. Hernia 2010;14:389-95
- Amato G. et al. A new shape of mesh to simplify and standardize the implantation procedure in ventral hernia repair. Hernia 2010;14:S-43
- Amato G. et al. Fixation free open ventral hernia repair using a new mesh with integrated placement straps. Hernia 2011;15:S21
- Amato G. et al. New mesh shape and improved implantation procedure to simplify and standardize open ventral hernia repair. A preliminary report. Hernia 2011;5:659–665
- Amato G. et al. Fixation free prosthetic repair of large umbilical hernia granting a broad defect overlap. Hernia 2012;16: Sl43-S240
- Amato G. et al. Fixation free prosthetic repair of large umbilical hernia Hernia (2013) 17 (Suppl 2): S1-S26
- Amato G. et al. Tentacle‑shaped mesh for fixation‑free repair of umbilical hernias. Hernia. 2019 Aug;23(4):801-807