Femoral hernia
 This type of hernia, relatively infrequent, manifests in the femoral area (in the cranial part of Scarpa’s
This type of hernia, relatively infrequent, manifests in the femoral area (in the cranial part of Scarpa’s  triangle, inferior to the inguinal canal).
triangle, inferior to the inguinal canal).
It protrudes through the femoral ring, next to the major vessels of the thigh: the femoral artery and vein.
Due to the unique configuration of the female pelvis, it almost exclusively affects women, representing about 50% of all hernias in females. It rarely reaches large sizes and is often not easily reducible. Obstruction or strangulation is relatively common.
The conventional surgical treatment involves direct suturing and/or the placement of a static flat mesh. To prevent migration, flat meshes must be fixed to the surrounding tissues, which can exacerbate postoperative pain even weeks after the surgery. These flat meshes become incorporated by fibrotic scar tissue starting from a few weeks after implantation. The scar tissue after few months from the procedure shrink s the mesh. This type of biological response stiffens the mesh and can often lead to discomfort during movement.
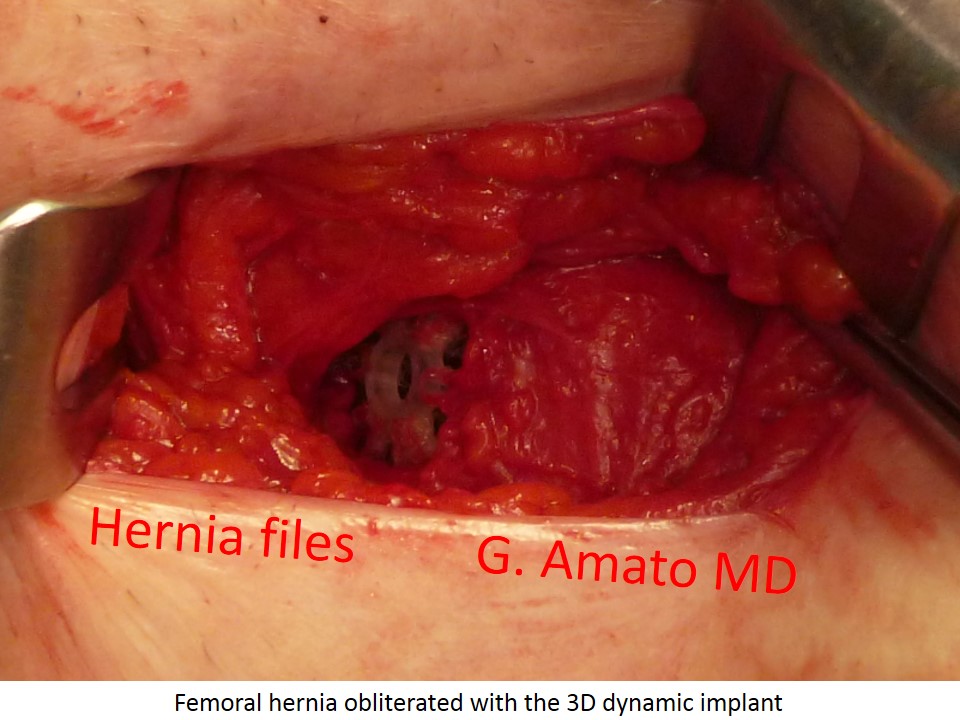
In contrast to the classical technique, Professor Amato developed an innovative fixation-free (sutureless) surgical technique with the 3D dynamic scaffold ProFlor. The procedure is usually performed under local anesthesia with excellent results, allowing patients to be discharged on the same day (day surgery) and achieves almost immediate postoperative recovery. The clinical results of this minimally invasive technique have been published and scientifically validated in the prestigious scientific journal International Journal of Surgery. (1)
The results of this advanced fixation free surgical approach are outstanding:
- Fast and safe mini-invasive approach
- Day surgery procedure carried out in local anesthesia in the vast majority of cases.
- Extremely low pain starting from the early postoperative stage
- Return to normal activities within one week
- Complication rate near to zero
Reference:
- Amato G. at al. Fixation free femoral hernia repair with a 3D dynamic responsive implant. A case series report. Int J Surg. 2018 Jun;54(Pt A):70-75